Ultrasound Monitorig
for Your IVF Cycle
For IVF monitoring cycles that are out-of-state of your location
Starting your cycle
Starting an IVF cycle is stressful enough, doing it with an out-of-state provider just increases that stress. That is why we have developed an out-of state monitoring program to help women that need ultrasound monitoring without having to travel to their provider. We follow your physicians instructions and with be able to accommodate your schedule. Most all cycles, whether retrievals or transfers, will need 2-3 ultrasounds during that cycle. All reports can be faxed or emailed to your physician within 2-3 hours after the exam is finished.
To schedule an appointment
Please Call True Health Acupuncture at 702-475-0870
You can also book online on the True Health Acupuncture website.
1481 W Warm Spring Rd #129
Henderson, Nevada 89014
Testimonials
My name is Michelle Aukerman. And I just have to say that Joyce at True Health Acupuncture is probably the best ultrasound technician I have ever had in my life and I’ve been through several. She’s very personal and talks through everything and if something goes wrong, she says OK how do we make this right? What’s the next step we need to take? You don’t hear that from any other ultrasound tech, they're so jaded. The comfort environment at True Health Acupuncture is unmatchable. It does not feel like a doctor's office and everybody is so warm but when it comes to Joyce, she is completely unmatched. It’s like having your own mother right there with you. I highly highly recommend her.
Thank you, the Aukerman’s
Michelle A.
This is the second pregnancy that I came to Joyce for my outside monitoring. I have been very nervous about the whole process, but Joyce guided me through each and every ultrasound. Although the monitoring went smoothly, upon achieving pregnancy I developed some bleeding. Of course, I panicked. Joyce explained everything that was going on with my bleeding and helped me through this anxious time. I don’t know what I would have done without Joyce’s calm demeanor. And the added bonus is having acupuncture treatment right there at True Health Acupuncture, the office Joyce works out of. I will always be truly thankful for the amazing experience that I received from both Joyce and True Health to be a part of my fertility journey.
Sara P.
Joyce is an exceptional individual who made a significant impact during my IVF journey. I had the privilege of meeting her when I needed support, and she was able to perform ultrasounds when our IVF Dr was unable to accommodate us. Her ability to confirm our twin pregnancy was incredibly reassuring. Joyce took the time to explain everything she was observing, which not only made the experience more memorable but also helped alleviate my anxiety. Her compassionate approach truly made a difference in my experience.

Nicole B
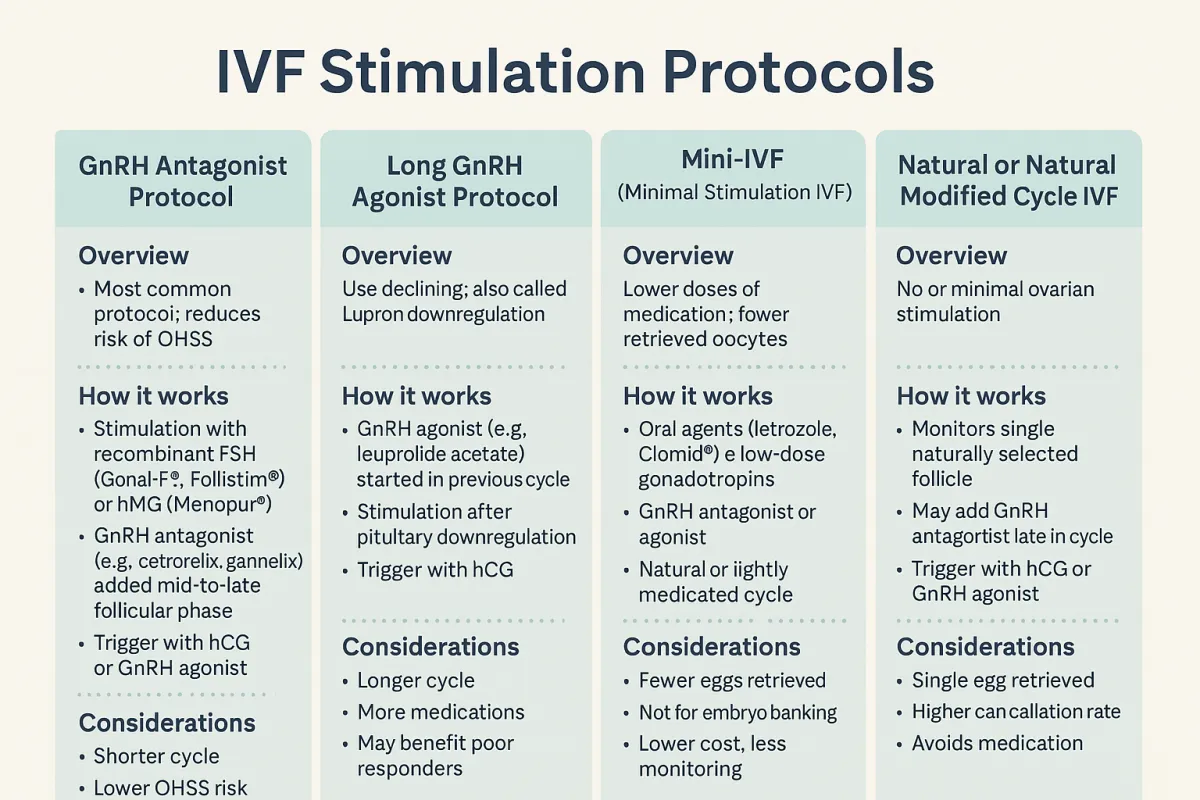
IVF Stimulation Protocols – Choosing the Right Approach
In modern IVF, ovarian stimulation is not one-size-fits-all. A variety of protocols are used based on age, ovarian reserve, past response, hormone levels, and individual goals. Here’s a breakdown of the most widely used stimulation strategies.
1. GnRH Antagonist Protocol (Flexible or Fixed Start)
Overview:
Now the most common IVF stimulation protocol in the U.S., the antagonist protocol is appreciated for its flexibility and reduced risk of ovarian hyperstimulation syndrome (OHSS).
How it works:
Stimulation begins: Day 2 or 3 of cycle with recombinant FSH (Gonal-F®, Follistim®) or hMG (Menopur®).
GnRH antagonist (e.g., cetrorelix, ganirelix) is introduced on day 5–6 or when the lead follicle reaches ~14 mm.
Trigger: Final maturation is triggered with either hCG (Pregnyl®, Ovidrel®) or a GnRH agonist (e.g., Lupron®) in high responders.
Advantages:
Shorter cycle length
Lower OHSS risk
Preferred in PCOS patients and egg donors
2. Long GnRH Agonist Protocol (Lupron Downregulation)
Overview:
Once the standard protocol, now used selectively—often for endometriosis or poor responders.
How it works:
GnRH agonist (e.g., leuprolide acetate): Started in the mid-luteal phase of the cycle prior to stimulation to suppress natural hormone fluctuations.
Stimulation begins after full pituitary downregulation (~10–14 days).
Trigger: Typically hCG.
Advantages:
More synchronized follicular growth
May improve implantation rates in specific subgroups
Drawbacks:
Longer and more intense
Risk of over-suppression in some patients
3. Mini-IVF (Minimal Stimulation IVF)
Overview:
Uses lower doses of medication with the goal of retrieving fewer, higher-quality eggs.
How it works:
Oral agents like letrozole or Clomid®, sometimes paired with low-dose gonadotropins
GnRH antagonist or agonist used for suppression
Often used in natural or lightly medicated cycles
Ideal for:
Poor responders
Older patients
Patients seeking lower-cost or lower-risk cycles
Limitations:
Fewer eggs retrieved
Not ideal for embryo banking
4. Natural or Natural Modified Cycle IVF
Overview:
No ovarian stimulation or very minimal drug use. Monitors and retrieves the single naturally selected follicle.
How it works:
Monitoring via ultrasound and labs
Possible use of GnRH antagonist late in the cycle
Trigger with hCG or GnRH agonist
Used when:
Avoiding medications
High risk for OHSS
Specific religious/philosophical beliefs
Limitations:
Single egg retrieval
Higher cycle cancellation rate
Tailoring the Protocol
Your reproductive endocrinologist chooses the protocol based on:
Antral follicle count (AFC) and AMH levels
Age and previous IVF response
Diagnosis (e.g., PCOS, diminished ovarian reserve)
Risk of OHSS
Patient preference and treatment goals